On May 31, Revolution Medicines presented the full Phase 3 RASolute 302 dataset at the ASCO plenary in Chicago, simultaneously published in the New England Journal of Medicine. Daraxonrasib cut the risk of death by 60%. The drug produced a 33.2% objective response rate versus 11.8% on chemotherapy and nearly halved the rate at which patients' pain worsened.
On June 8, Tango Therapeutics reported that vopimetostat, an experimental PRMT5 inhibitor, combined with daraxonrasib produced a 92% objective response rate in MTAP-deleted, RAS-mutant pancreatic cancer. Ninety percent of patients remained progression-free at six months. Revolution Medicines is preparing its NDA under the Commissioner's National Priority Voucher program; the CNIO triple-therapy paper, retracted in April for undisclosed financial ties, remains in peer review.
Why it matters
Daraxonrasib is the first drug to beat chemotherapy in a Phase 3 trial for pancreatic cancer, where five-year survival sits at 13%.
Questions about this story
0
I guess that sounds good, but 13 months is not what I would call a success. Did it cure any of the subjects?
No cures — but 'median' survival of 13.2 months means half the patients lived longer, and a hazard ratio of 0.40 is unusually strong for a disease where second-line chemo typically buys 4–5 months.
Why it matters: This is previously treated metastatic pancreatic cancer — historically one of medicine's most treatment-resistant diagnoses — where 'cure' has never been a realistic endpoint; the question is how many more months, not whether cancer disappears.
—Objective response rate was roughly 35% in G12-mutant patients on 300 mg — meaning about a third had measurable tumor shrinkage, but complete responses (full disappearance) were not reported as a meaningful category.
—The hazard ratio of 0.40 means patients on daraxonrasib had 60% lower odds of dying at any given moment versus chemo — that kind of effect size is what oncologists mean when they call a result 'unprecedented' for this disease.
—Median is the midpoint: half of patients died before 13.2 months, half lived longer — some potentially far longer. The shape of the survival curve's tail, which ASCO full data may show, matters as much as the median.
—The standard of care for second-line metastatic pancreatic cancer (nanoliposomal irinotecan-based regimens) has historically yielded medians around 6–6.7 months — so 13.2 months is roughly a doubling, not a marginal gain.
Some oncologists argue that a 60% hazard reduction is a paradigm shift deserving the 'unprecedented' label Revolution Medicines used; skeptics counter that 13.2-month median survival still means most patients die within two years, and durable remissions — let alone cures — remain vanishingly rare in metastatic PDAC regardless of the drug.
AI-generated with web search — may be wrong. Check the linked sources.
Images from Openverse under Creative Commons licenses.
Videos from YouTube.
Voices
Curated perspectives — historical figures and your fellow readers.
Oscar Wilde
(1854-1900) ·Victorian · wit
Fictional AI pastiche — not real quote.
"How delightful that Science, having spent forty years declaring something impossible, has finally succeeded by the simple expedient of trying three times as hard—a strategy that would have saved many a Victorian marriage, had anyone thought to apply it. One does hope the mice appreciate being cured of their mortality, though I suspect they would have preferred never to have been given cancer in the first place."
100% found this insightful
Ever wondered what historical figures would say about today's headlines?
Sign up to generate historical perspectives on this story.
19 events
Latest: May 22nd, 2026 · 3 weeks ago
Showing 8 of 19
JK to step
Tap a bar to jump to that date
Jump to
May 2026
Revolution Medicines Pre-Announces 'Positive' Phase 3 Results Before ASCO
LatestBusiness
Revolution Medicines announces a post-ASCO investor conference call for May 31 at 7:00 PM ET, describing RASolute 302 results as "positive" in a public filing—the company's first use of that characterization ahead of the plenary presentation.
NEJM Publishes Phase 1/2 Daraxonrasib Data
Research
The New England Journal of Medicine publishes Phase 1/2 trial results for daraxonrasib in 168 patients with previously treated RAS-mutated pancreatic cancer, detailing the efficacy and safety data that supported the Phase 3 design.
Revolution Medicines Raises $2.225 Billion
Business
Revolution Medicines reports Q1 2026 results and discloses $2.225 billion raised in April capital offerings—$1.725 billion in common stock and $500 million in convertible notes—to fund the daraxonrasib NDA and an expanded Phase 3 pipeline across pancreatic, lung, and colorectal cancers.
Barbacid Divests from Vega Oncotargets
Research
Barbacid returns his shares (valued at 750 euros) and two patent applications to Vega Oncotargets, severing commercial ties with the spin-off to prevent the conflict-of-interest dispute from affecting the resubmitted triple-therapy paper.
April 2026
FDA Authorizes Expanded Access for Daraxonrasib
Regulatory
The FDA issues a safe-to-proceed letter for a daraxonrasib expanded access program, allowing patients with previously treated metastatic pancreatic cancer to receive the drug outside a clinical trial while the NDA is prepared.
PNAS Retracts CNIO Triple-Therapy Paper
Research
PNAS retracts the January 2026 Barbacid study, citing an undisclosed competing interest: Barbacid, Carmen Guerra, and Vasiliki Liaki held financial stakes in Vega Oncotargets, a spin-off they co-founded in 2024 to commercialize the therapy. Editors stated no errors were found in the underlying science; the authors plan to resubmit through standard peer review with full disclosure.
Phase 3 Data Selected for ASCO Plenary Session
Research
Revolution Medicines announces the RASolute 302 results will be presented in a Plenary Session at the ASCO Annual Meeting in Chicago on May 31, 2026—a slot reserved for the most significant oncology trial findings of the year.
Revolution Medicines announces positive topline results from the Phase 3 RASolute 302 trial: daraxonrasib extended median overall survival to 13.2 months versus 6.7 months on chemotherapy, with a hazard ratio of 0.40 (p<0.0001), cutting death risk by 60%.
CNIO publishes PNAS study showing complete and lasting pancreatic tumor elimination in mice using daraxonrasib plus afatinib plus SD-36. Nine of 12 genetically modified mice achieved full regression; implanted tumor models remained cancer-free for 250+ days.
Merck Acquisition Talks Collapse
Business
Negotiations between Merck and Revolution Medicines over a potential $28-32 billion acquisition ended without agreement on price. Revolution Medicines stock dropped 20% following the announcement, erasing nearly $6 billion in market value.
Merck Enters Acquisition Talks
Business
Financial Times reports Merck in talks to acquire Revolution Medicines for $28-32 billion, potentially making it the largest biotech deal since Pfizer's $43 billion Seagen acquisition in 2023. Stock surged 20% on the news.
Daraxonrasib Monotherapy Shows Survival Gains
Research
Early reporting from Phase 1 trials shows daraxonrasib nearly doubles median survival to 15.6 months compared to 7 months with standard chemotherapy, with more than 90% of 83 patients experiencing disease stabilization and roughly 30% seeing tumor shrinkage.
October 2025
Daraxonrasib Receives Orphan Drug Status
Regulatory
FDA grants Orphan Drug Designation to daraxonrasib for pancreatic cancer treatment, providing additional development incentives.
July 2025
Daraxonrasib Gets Breakthrough Designation
Regulatory
FDA grants Breakthrough Therapy Designation to daraxonrasib (RMC-6236), a multi-selective KRAS inhibitor that targets mutations common in pancreatic cancer, based on promising Phase 1 data showing 8.8-month progression-free survival.
December 2022
Second KRAS Inhibitor Approved
Regulatory
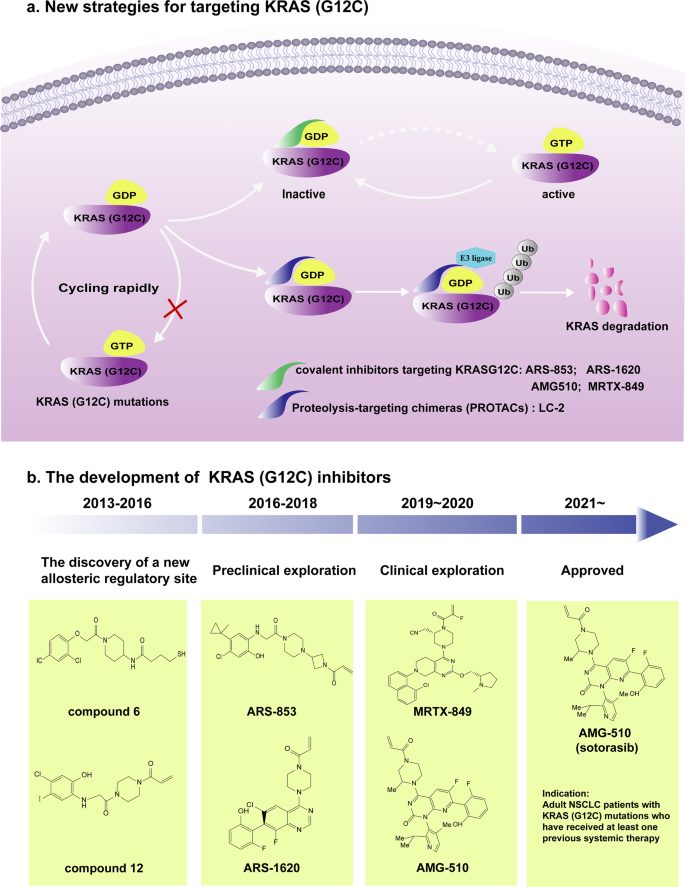
FDA approves adagrasib (Krazati) for KRAS G12C-mutated lung cancer, providing a second option but still not addressing the G12D mutations dominant in pancreatic cancer.
May 2021
First KRAS Inhibitor Approved
Regulatory
FDA grants accelerated approval to sotorasib (Lumakras) for KRAS G12C-mutated lung cancer—the first approved drug targeting any KRAS mutation after 40 years of failed attempts. However, G12C mutations are rare in pancreatic cancer.
November 2019
SD-36 STAT3 Degrader Published
Research
University of Michigan researchers publish SD-36, a PROTAC degrader that selectively destroys STAT3 protein. The compound achieves complete tumor regression in mouse models of leukemia and lymphoma.
July 2013
Afatinib Approved for Lung Cancer
Regulatory
FDA approves afatinib (Gilotrif), an irreversible EGFR inhibitor, for metastatic non-small cell lung cancer. This drug would later become one of three components in the CNIO triple therapy.
January 1982
First Human Oncogene Isolated
Discovery
Three independent research groups, including Barbacid's, identify HRAS as the first human oncogene. The discovery establishes RAS proteins as central to cancer but also reveals how difficult they are to drug.
Historical Context
3 moments from history that rhyme with this story — and how they unfolded.
1 of 3
May 2001
Imatinib and Chronic Myeloid Leukemia (2001)
The FDA approved imatinib (Gleevec) for chronic myeloid leukemia, the first cancer drug designed to target a specific molecular defect—the BCR-ABL fusion protein. Patients who had months to live began achieving long-term remission. The drug transformed CML from a death sentence into a manageable chronic condition.
Then
Five-year survival for CML patients jumped from 30% to over 90%.
Now
Imatinib became the template for targeted cancer therapy, proving that attacking specific oncogenic drivers could succeed where chemotherapy failed.
Why this matters now
KRAS researchers explicitly cite imatinib as their model. Like BCR-ABL, KRAS drives cancer growth; unlike BCR-ABL, KRAS resisted drugging for 20 additional years. The CNIO triple therapy aims to achieve for pancreatic cancer what imatinib did for CML.
2 of 3
2003-2013
EGFR Inhibitors in Lung Cancer (2003-2013)
After early EGFR inhibitors showed mixed results in unselected lung cancer patients, researchers discovered that only tumors with specific EGFR mutations responded. Gefitinib (2003) and erlotinib (2004) were approved for mutation-positive patients, followed by afatinib (2013). However, resistance typically emerged within 12-18 months.
Then
EGFR-mutant lung cancer patients gained months to years of progression-free survival.
Now
The resistance problem drove development of next-generation inhibitors and combination strategies—the same approach now being applied to KRAS.
Why this matters now
Afatinib, one of the three drugs in the CNIO combination, was designed to overcome resistance to earlier EGFR inhibitors. The triple therapy strategy—blocking the primary driver plus escape routes—directly responds to lessons learned from EGFR resistance.
3 of 3
May 2021
KRAS G12C Breakthrough (2021)
After researchers discovered a previously unknown binding pocket on the KRAS G12C mutant protein, Amgen developed sotorasib—the first approved drug targeting any KRAS mutation. The FDA granted accelerated approval based on a 36% response rate in lung cancer patients who had failed other treatments.
Then
Patients with G12C mutations gained a new treatment option, though responses were often temporary.
Now
The approval proved KRAS was druggable after all, triggering massive investment in inhibitors targeting other KRAS mutations.
Why this matters now
Sotorasib's approval validated the KRAS-targeting approach but left pancreatic cancer patients behind—G12C mutations occur in only 1-2% of pancreatic tumors versus 40% for G12D. The CNIO study uses daraxonrasib, which targets the mutations actually common in pancreatic cancer.