0
How does it work?
IgA nephropathy is driven by abnormal antibodies that lodge in the kidney; JADE101 blocks the protein (APRIL) that tells immune cells to make those antibodies, cutting their production by ~70% after a single shot.
Why it matters: Interrupting the disease earlier in the chain — before the abnormal IgA is even made — is a fundamentally different bet than the older approved drugs, which mostly reduce kidney pressure downstream.
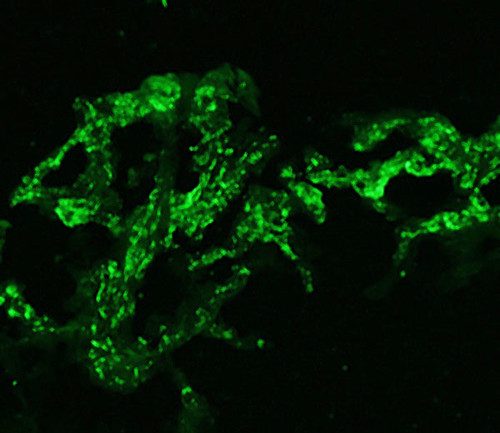
- The disease follows a 'four-hit' cascade: immune cells overproduce galactose-deficient IgA1 (an abnormal antibody), autoantibodies form immune complexes with it, those complexes deposit in the kidney's mesangium, and inflammation erodes kidney function over years.
- APRIL (A Proliferation-Inducing Ligand) is the cytokine that drives B-cells to produce and class-switch toward pathogenic IgA1; blocking it upstream stops the cascade at its source — JADE101 binds APRIL with ultra-high affinity to do exactly that.
- Jade engineered JADE101 for half-life extension, giving it a serum half-life of ~27 days; that's why a single dose suppresses IgA for 12 weeks, versus monthly dosing for Otsuka's sibeprenlimab (Voyxact), which shares the same APRIL-blocking mechanism.
- The other four approved drugs act on downstream effects: budesonide (Tarpeyo) reduces mucosal IgA at gut lymph nodes, sparsentan (Filspari) and atrasentan (Vanrafia) cut kidney pressure via receptor blockade, and iptacopan (Fabhalta) blocks the complement system that amplifies kidney inflammation.
Room for disagreement
- Jade claims a 'best-in-class' edge over Voyxact (sibeprenlimab) based on tighter APRIL binding and longer half-life — but sibeprenlimab has actual patient trial data (VISIONARY: 54% proteinuria reduction) while JADE101's 70% IgA cut comes only from healthy volunteers, where the pathological milieu driving IgA overproduction is absent. Critics would note healthy-volunteer pharmacodynamics don't guarantee equivalent suppression in diseased patients.
AI-generated with web search — may be wrong. Check the linked sources.